West German Infection Prevention Network - AI-based antibiotic resistance detection
Antimicrobial resistance is also known as the “silent pandemic”, which claims up to 5 million lives every year. Targeted and early antibiotic therapy can save lives in case of serious infections. Until now, the traditional methods of medical microbiology have a long turnaround time. Faster methods are therefore urgently needed. In the "Westdeutsches Infektionspräventionsnetzwerk - KI-basierte Antibiotikaresistenzdetektion" (WIN-KID), we want to investigate whether whole genome data are suitable for detecting not only antibiotic resistance but also the so-called “minimal inhibitory concentrations” (MIC) of antibiotics. This has two advantages over the pure prediction of resistance: Firstly, the predictions are independent of updated in the MIC interpretation guideline; secondly, with the knowledge of the MIC, the dose of antibiotics can be better adjusted in severe infections. The prediction of the MIC is to be tested using machine learning. To this end, partners from microbiology, hygiene, bioinformatics/artificial intelligence and SMEs are cooperating in the WIN-KID network in order to improve healthcare in the long term, not only in NRW.
Predicting antimicrobial resistance with machine learning algorithms
The emergence and spread of antimicrobial resistance is a global concern as it is causing an increasing number of deaths (approx. 4.95 million in 2019). To curb this development, the use of antimicrobials must be reduced or more targeted. Currently, the rational use of antimicrobials is limited by slow diagnostic methods. Rapid antimicrobial susceptibility testing methods are therefore needed.
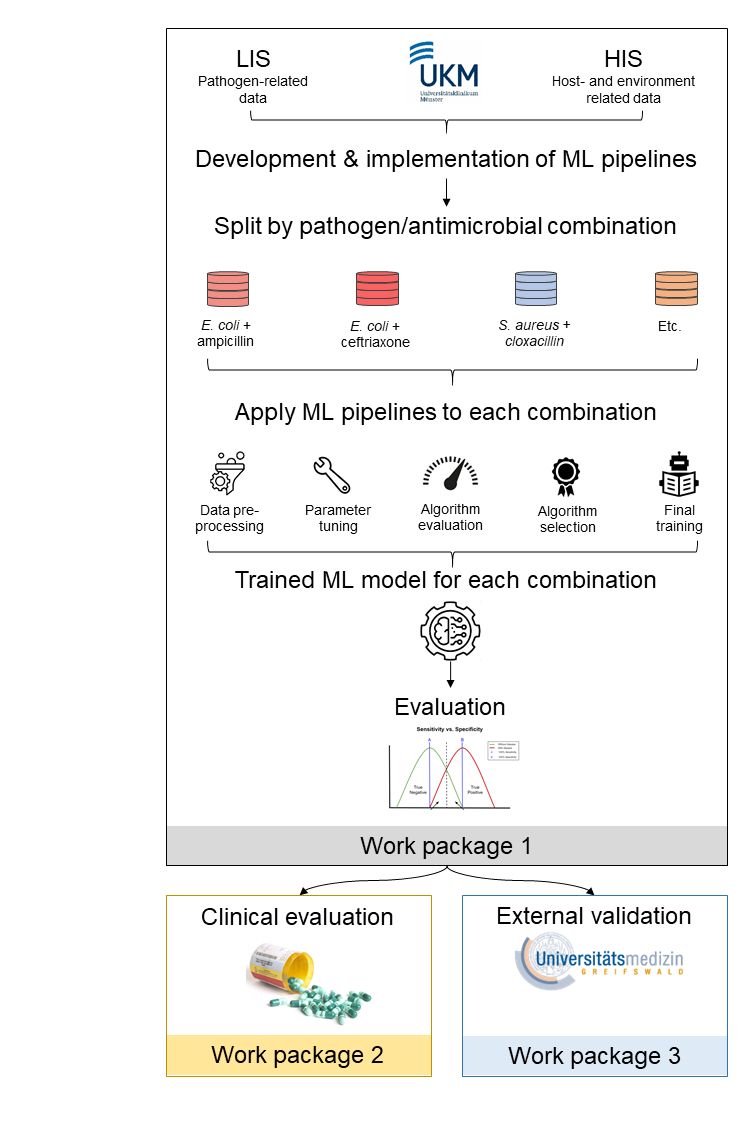
The risk of infection with antimicrobial-resistant pathogens is not only determined by the pathogen itself (e.g. resistance genes), but also by the host/human (e.g. drugs, pre-existing diseases) and the environment (occupational exposure in farmers, nursing home residences). We therefore want to investigate whether holistic information from pathogen, patient, and environmental data can be used to accurately predict antimicrobial resistance using machine learning (ML) methods. This prediction would be available immediately after species identification, 18–24 h earlier than culture-based methods. Our project also differs from other work in that we aim to predict the exact minimum inhibitory concentration (MIC) rather than just resistance. The MIC is independent of the steadily changing MIC breakpoints at which a pathogen is considered resistant, so our proposed models could be used in a generalized fashion.
We will create a project-specific retrospective database of patients treated for bacterial infection at Münster University Hospital (2021–2022). We will fit and compare different ML models for each combination of species and antimicrobial, including random forests, extreme gradient boosting, support vector machines, regularized linear regressions, and neural networks. Each model consists a pipeline including preprocessing, variable selection, etc., whose hyperparameters are optimized. The goal is to identify the best ML model and the most important influencing variables and to approximate it by a less complex (sparse) model that can be used in clinical practice. We will validate the generalizability of the predictive ability of the final ML models on a separate dataset from another geographic region in Germany.
In a retrospective patient population, we will test whether predicting antimicrobial resistance using ML algorithms would have improved antimicrobial prescribing. For this purpose, the predicted MICs will be translated into the categories "susceptible", and "resistant" using EUCAST breakpoints. We will compare the ML-based prediction with the prescription of the medical staff.
Using the proposed study, we can contribute to the extent to which ML algorithms can be integrated into microbiological diagnostics to improve antimicrobial prescribing by using pathogen, patient, and environmental data. The project is funded by the German Research Foundation (SCHA 1994/12-1)
Improving the treatment of skin and soft tissue infections in Low and Middle Income Countries
At Masanga Hospital in Sierra Leone, we are currently conducting a research project to improve the care of skin and soft tissue infections. Staphylococcus aureus strains in sub-Saharan Africa often produce the pore-forming protein toxin "Panton-Valentine Leukocidin". We want to test whether the toxin effect can be attenuated by the additional administration of clindamycin in the treatment of S. aureus infections. This project is supported by the Gesellschaft für Internationale Zusammenarbeit/Else-Kröner Fresenius Stiftung.
Care of Buruli ulcer patients in Sierra Leone
Buruli ulcer is caused by Mycobacterium ulcerans, but the pathogen is very difficult to detect. At Masanga Hospital in Sierra Leone, patients with Buruli ulcer are treated in a special consultation. We want to support medical care by establishing a PCR-based rapid diagnostic test on site. This project is supported by the Gesellschsaft für Internationale Zusammenarbeit / Else-Kröner Fresenius Stiftung. You can also find more information about the project here.
Transmigration of Staphylococcus aureus from blood to urine: a route to early sepsis diagnosis?
Patients with Staphylococcus aureus bacteremia (SAB) can have concomitant S. aureus bacteriuria (SABU), which is associated with a worse clinical outcome. Together with our collaborative partners from the Core Unit Proteomics (Prof. Simone König), we aim to understand how transmigration of S. aureus from blood to urine occurs and whether this phenomenon of secondary SABU can be exploited for a "point-of-care" detection of SAB. The urine proteome of individuals with SAB and non-S. aureus bacteremia will be compared with respect to S. aureus specific proteins. This should identify antigen candidates that could be used for the development of a rapid lateral flow test. The project is funded by the German Research Foundation (SCHU 3689/1-1).