
Copy number alteration (CNA)Department of Paediatric Haematology and Oncology, University Hospital Muenster, Muenster, GermanyAIM OF THE PROJECT
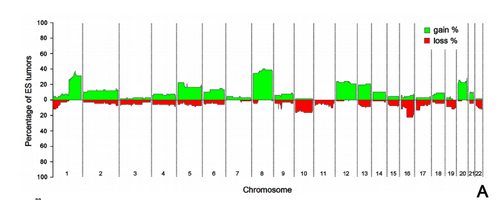
Copy number alterations are common events in ES. Previous work from our consortium and others reported an impact of CNAs on ES clinical outcome. Most recently, the relevance of chromosome (chr) 1q gain (1qG), chr 8q and 20 gains10, loss of chr 16q, and alteration of p53 and p16/p14ARF were described as relevant negative prognostic CNAs in this neoplasm. These biomarkers were significant in multivariate analysis, which did include the classical prognostic parameters. These studies were performed in retrospective series of ES patients and there is a clear need for a prospective validation. Integrative genomic and functional analyses showed several candidate genes in particular regions, i.e., CDT2 and PARP1 in chr 1q or MTDH (metadherin, AEG-1) in chr 8, which are amenable to targeted therapy. ). Our research goal is novel in that we aim to establish prospectively the clinical value of CNAs in ES patients and illustrate the potential importance of genetic alterations for risk stratification. The study will be complemented by exome sequencing (►WP1.2) and genome-wide association studies embedded in ongoing research, e.g. within TranSaRNet and ASSET.
Copy number alterations are common events in ES. Previous work from our consortium and others reported an impact of CNAs on ES clinical outcome. Most recently, the relevance of chromosome (chr) 1q gain (1qG), chr 8q and 20 gains10, loss of chr 16q, and alteration of p53 and p16/p14ARF were described as relevant negative prognostic CNAs in this neoplasm. These biomarkers were significant in multivariate analysis, which did include the classical prognostic parameters. These studies were performed in retrospective series of ES patients and there is a clear need for a prospective validation. Integrative genomic and functional analyses showed several candidate genes in particular regions, i.e., CDT2 and PARP1 in chr 1q or MTDH (metadherin, AEG-1) in chr 8, which are amenable to targeted therapy. ). Our research goal is novel in that we aim to establish prospectively the clinical value of CNAs in ES patients and illustrate the potential importance of genetic alterations for risk stratification. The study will be complemented by exome sequencing (►WP1.2) and genome-wide association studies embedded in ongoing research, e.g. within TranSaRNet and ASSET.
WORK PLAN
1) Validation process (Analytical validation): The purpose of this task is the systematic evaluation of the specificity, sensitivity, accuracy and reproducibility of a robust, simple and cost-effective approach such as an interphase FISH (analysis) (iFISH) for prospective validation of CNA. We will develop and validate iFISH probes for i) relevant regions for prospective validation chr 1q, chr16, and ii) for relevant genes, such as CDT2 and PARP1 which will be analysed exploratory. iFISH will be performed on the same paraffin-embedded tissues used for the analyses described below. The purpose of FISH analyses is: i) to validate a robust, cost-effective, quick and simple tool, iFISH, which is available in every surgical pathology laboratory, and ii) to help provide a standard for the systematic evaluation of the specificity, sensitivity, accuracy and reproducibility of the Affymetrix OncoScanTM technique (see task 2, immediately below).
2) Biomarker qualification (Early clinical validation): The purpose of this task is to explore and assess the sensitivity and specificity of genome-wide CNA screening for clinical end-point determination (event-free survival and overall survival) and the assessment of its clinical utility. Our analysis on prospectively collected patient material will focus on the validation of 1q gain and 16q loss and will be complemented by an exploratory analysis of CNA. Copy number, genotypic and somatic mutation analyses will be carried out using the Affymetrix OncoScanTM FFPE Express 2.0 with more than 335,000 markers relevant in cancer. These markers include: 201 tumour suppressor genes, genes and mutations of the PI3K pathway, and more than 400 somatic mutations.
We will use the same samples for the validation of other biomarkers (►WP3). The proposed analysis is complementary to ►WP1.2. We will provide, at relatively low cost, complementary and robust information with respect to that provided by other groups of the proposal. Importantly, this can be done on formalin-fixed paraffin-embedded tissues, the routine format of clinical samples, which ensures the feasibility of its routine clinical implementation.
EXPLOITATION OF THE RESULTS
At present, clinical prognostic factors such as stage, tumour size and response to induction chemotherapy are used for the stratification of patients into different risk groups. The outcome in ES patients has not significantly improved in the past two decades. Current standard therapies, which combine high-intensity chemotherapy, surgery and radiotherapy, also put patients at risk of severe longterm sequelae. It is our aim to develop new, complementary models for stratification based on biological biomarkers. The new stratification criteria including predictive biomarkers will open the door to better individual risk-adapted therapies and will improve cure rates and the quality of cure. Furthermore, there is a chance of bringing novel targeted therapies into the treatment of ES. Patient selection by the use of validated predictive and/or prognostic biomarkers may eventually help to increase the cost effectiveness of treatment by a) early detection of non-responders, who will then be switched to a more effective treatment and b) reduction of treatment-induced long-term morbidity in patients who are eligible for less intense treatments and c) identification of patients at risk who are a target group for new treatment strategies. In many European countries, the value of novel medical diagnostics or treatments is assessed by relating its cost to the quality of life (“QALY”) of a patient. The prerequisite for such a rating would be the implementation of treatment stratification according to the biomarker signatures that we aim to identify.
1) Validation process (Analytical validation): The purpose of this task is the systematic evaluation of the specificity, sensitivity, accuracy and reproducibility of a robust, simple and cost-effective approach such as an interphase FISH (analysis) (iFISH) for prospective validation of CNA. We will develop and validate iFISH probes for i) relevant regions for prospective validation chr 1q, chr16, and ii) for relevant genes, such as CDT2 and PARP1 which will be analysed exploratory. iFISH will be performed on the same paraffin-embedded tissues used for the analyses described below. The purpose of FISH analyses is: i) to validate a robust, cost-effective, quick and simple tool, iFISH, which is available in every surgical pathology laboratory, and ii) to help provide a standard for the systematic evaluation of the specificity, sensitivity, accuracy and reproducibility of the Affymetrix OncoScanTM technique (see task 2, immediately below).
2) Biomarker qualification (Early clinical validation): The purpose of this task is to explore and assess the sensitivity and specificity of genome-wide CNA screening for clinical end-point determination (event-free survival and overall survival) and the assessment of its clinical utility. Our analysis on prospectively collected patient material will focus on the validation of 1q gain and 16q loss and will be complemented by an exploratory analysis of CNA. Copy number, genotypic and somatic mutation analyses will be carried out using the Affymetrix OncoScanTM FFPE Express 2.0 with more than 335,000 markers relevant in cancer. These markers include: 201 tumour suppressor genes, genes and mutations of the PI3K pathway, and more than 400 somatic mutations.
We will use the same samples for the validation of other biomarkers (►WP3). The proposed analysis is complementary to ►WP1.2. We will provide, at relatively low cost, complementary and robust information with respect to that provided by other groups of the proposal. Importantly, this can be done on formalin-fixed paraffin-embedded tissues, the routine format of clinical samples, which ensures the feasibility of its routine clinical implementation.
EXPLOITATION OF THE RESULTS
At present, clinical prognostic factors such as stage, tumour size and response to induction chemotherapy are used for the stratification of patients into different risk groups. The outcome in ES patients has not significantly improved in the past two decades. Current standard therapies, which combine high-intensity chemotherapy, surgery and radiotherapy, also put patients at risk of severe longterm sequelae. It is our aim to develop new, complementary models for stratification based on biological biomarkers. The new stratification criteria including predictive biomarkers will open the door to better individual risk-adapted therapies and will improve cure rates and the quality of cure. Furthermore, there is a chance of bringing novel targeted therapies into the treatment of ES. Patient selection by the use of validated predictive and/or prognostic biomarkers may eventually help to increase the cost effectiveness of treatment by a) early detection of non-responders, who will then be switched to a more effective treatment and b) reduction of treatment-induced long-term morbidity in patients who are eligible for less intense treatments and c) identification of patients at risk who are a target group for new treatment strategies. In many European countries, the value of novel medical diagnostics or treatments is assessed by relating its cost to the quality of life (“QALY”) of a patient. The prerequisite for such a rating would be the implementation of treatment stratification according to the biomarker signatures that we aim to identify.